
Over the weekend, I spoke to a close friend, and she shared that her 75-year-old aunt, a three-time cancer survivor with preexisting conditions, was struggling to acquire a dose of the COVID-19 vaccine in her home state of Florida. Unfortunately, Florida allows healthy individuals who are frustrated with the rate of vaccine distribution in their own states to be vaccinated, even before individuals like my friends’ aunt. This is just a single instance of how the lack of organization and regulation in some states’ COVID-19 vaccine rollout plans is impacting those who are in the greatest need of the vaccine.
While former President Trump’s Operation Warp Speed facilitated the development of an efficacious COVID-19 vaccine on an accelerated timeline, it fell flat when it came time to administer those doses to the American public. President Biden has laid out a plan to administer 100 million doses in the first 100 days of his term.
After the loss of more than 2 million lives worldwide, multiple periods of quarantine, and an upheaval of life as we’ve known it for the past few decades, President Biden’s plan may feel like a panacea for the frustration and restlessness that many feel. However, the speed of this vaccine rollout plan does not ensure a quicker return to normalcy, and it may be sacrificing equity for the sake of efficiency.
Inequity of Nationwide Vaccine Rollout Plans
There is little question that the COVID-19 pandemic has disproportionately affected African American and Hispanic communities in the United States. However, as vaccine distribution has ramped up, vaccination patterns in the 17 states that are publicly reporting COVID-19 vaccination data are not reflective of who the virus has affected the most.
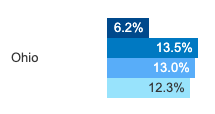
Simply put, the groups that have been hit the hardest by the COVID-19 pandemic are the ones who are not receiving the vaccines. For example, in my home state of Ohio, while African Americans account for 13.5 percent of COVID-19 cases and 13 percent of COVID-related deaths, only 6.2 percent of African Americans have been vaccinated as of Jan. 19, 2021. In comparison, Caucasians in Ohio account for 74 percent of COVID-19 cases and 82 percent of COVID-19 deaths, and 83 percent of Caucasians have been vaccinated as of Jan. 19, 2021. There is a 1 percent difference between the number of Caucasians who have been diagnosed with COVID-19 and those who have been vaccinated, while there is a 6.8 percent difference between the number of African Americans who have been diagnosed with COVID-19 and those who have been vaccinated.
A similar trend has emerged in a number of the other 17 states, such as Florida and Tennessee, that are publicly reporting their COVID-19 vaccination data.
![]()

The disparities observed in the graphs above can be attributed to a few factors. The most significant of these factors is the mistrust, which stems from decades of structural racism, that African American and Hispanic communities harbor for the American healthcare system. A Quest Diagnostics Health Trends ™ analysis found that only 64 percent of African Americans and 67 percent of Hispanics, compared to 84 percent of Caucasians, believe that they would receive the same life-saving care as their Caucasian counterparts if diagnosed with COVID-19. These groups also lack confidence that they will have access to the COVID-19 vaccine, and rightfully so. There are consistently fewer vaccination sites in regions where African American and Hispanic populations are concentrated. For instance, low income neighborhoods in the Houston area have been deemed “pharmacy deserts” by Dr. Peter Hotez, Dean of the National School of Tropical Medicine at Baylor College of Medicine. In a similar vein, individuals in these regions often do not have access to transportation, so they are also unable to get to vaccination sites that are farther away.
Vaccine Rollout from a Global Perspective
Disparities in vaccine distribution and access are not localized to the United States – they extend across the globe. For instance, officials who are working towards acquiring doses for the continent of Africa anticipate that they will have to wait weeks, if not months, before receiving World Health Organization-approved COVID-19 vaccines.
As of Jan. 22, 2021, the continent had procured enough vaccines to inoculate only around 30 percent of the African population. On the other hand, the United States has the purchase options to vaccinate each American five times over, while Canada has ordered enough vaccines to vaccinate each of its citizens six times over.
Vaccine shortages in developing countries can be attributed to the hoarding of supplies by affluent nations and funding shortfalls. The monopoly that these nations have on COVID-19 vaccines will affect not only impoverished countries, but also the countries that are hoarding the supplies.
For example, in the extreme situation that affluent countries have fully vaccinated their citizens, while citizens of developing countries remain largely unvaccinated, the global economy would suffer losses upwards of $9 trillion, with nearly half of this cost falling to affluent countries. The same study that posits this extreme scenario concludes that the equitable distribution of COVID-19 vaccines is in every country’s best interest because all economies are connected, and no single economy will recover until the others have recovered as well.
How Can the Vaccine Be Distributed More Equitably?
There are several ways to mitigate the disparities associated with COVID-19 vaccine distribution and access, some of which are outlined below:
- Treating Systemic Racism: While this is easier said than done, it is necessary to ensure that the groups who have been hit the hardest by the COVID-19 pandemic are willing to be vaccinated, when the resources are made available to them.
- Increasing Vaccination Sites: Ensuring that there are locations in close proximity to regions where African American and Hispanic communities are concentrated will increase the likelihood of these groups being vaccinated. Texas Health Resources recently launched an initiative to distribute the COVID-19 vaccine to the underserved region of Southeast Fort Worth. According to Dr. Catherine Oliveros, President of Community Health Improvement at Texas Health, they accomplished this by “[making] a commitment to go to their community, where they live, work, pray, and play and [making] the vaccine available to them there”.
- COVAX: A global initiative, backed by the World Health Organization (WHO), to ensure that the COVID-19 vaccine is accessible to all countries, regardless of their income level. On Jan. 22, 2021, Pfizer announced that it would provide 40 million doses to the WHO program at a “not-for-profit” price. This is a step in the right direction, but these doses are only a small fraction of those that will be required to vaccinate the 92 low and middle income countries that the WHO has pledged to support.
- Global Vaccine Sharing Program: Recently, India donated millions of doses of the AstraZeneca COVID-19 vaccine to its neighboring South Asian countries. Given the country’s position as the world’s largest vaccine producer, India will play a significant role in providing supplies to low and middle income countries.
- “Pro Bono” Vaccines: Canada has pledged to donate any remaining doses after it’s population has been vaccinated. While this is an admirable endeavor, it is important to note that low and middle income countries can not wait until other countries have been fully vaccinated or rely solely on a supply of donated vaccines.
These solutions aren’t perfect, but they are a step in the right direction towards eradicating racial disparities in the distribution of and access to the COVID-19 vaccine.

- Beef. It’s What’s Not for Dinner. – Plant-Based “Meat” and the Climate Crisis - January 16, 2022
- Activism or Slacktivism? Where ‘The Activist’ on CBS Went Wrong - September 17, 2021
- Combating Climate Change: The Great Green Wall - July 20, 2021